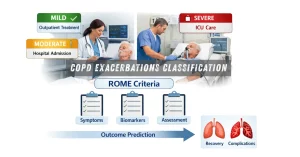
The ROME COPD exacerbation proposal works! Time to move forward
The ROME proposal for COPD exacerbations classification offers a new approach to assess severity and predict outcomes, improving clinical decision-making

COPD Management in Primary Care: Underutilisation of Nursing Consultations
Analysis of COPD management in primary care highlighting the role and underutilisation of nursing consultations and healthcare utilisation patterns in real-world patients.
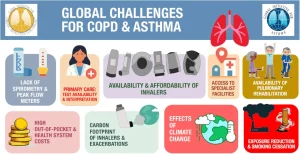
Addressing the Global Challenges of COPD and Asthma: A Shared Vision From the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) and the Global Initiative for Asthma (GINA)
Analysis of the global challenges of COPD and asthma and the shared vision of GOLD and GINA to improve diagnosis, access to inhaled therapies and patient outcomes worldwide.