

Climate change and respiratory health: implications for respiratory clinicians in primary and specialist care
Review on climate change and respiratory health, focusing on chronic respiratory diseases and implications for primary and specialist care.
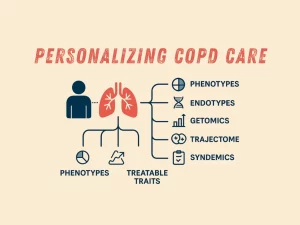
Personalizing COPD care: phenotypes, endotypes, GETomics, the the trajectome, syndemics and treatable traits
Discover how personalized COPD care integrates phenotypes, endotypes, GETomics, trajectome, syndemics, and treatable traits to improve patient outcomes.
TED Talk – The Invisible Epidemic
Jean Wright presents at TEDxCharlotte how millions live with COPD unknowingly. It’s time to identify and help the “missing millions.”

Climate Change & COPD: A GOLD Science Committee Review
Climate change and COPD are linked through extreme temperature, wildfire smoke, dust storms and allergen exposure, which pose major health threats.
Artificial Intelligence in COPD
Artificial Intelligence in COPD is transforming disease management, from underdiagnosis to treatment guidance. Discover how machine learning clusters patients, predicts outcomes, and optimizes healthcare resources.
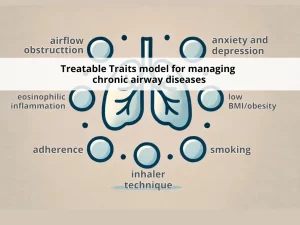
Change is in the air: key questions on the ‘Treatable Traits’ model for chronic airway diseases in primary care
Explore Treatable Traits model for chronic airway diseases like asthma and COPD in primary care. Learn about seven key traits — airflow obstruction, eosinophilic inflammation, adherence, inhaler technique, smoking, low BMI/obesity and anxiety and depression — that guide personalized care.